 A spinal tumor is a benign or cancerous growth of cells in the spinal cord or surrounding areas. These tumors can compress the spinal cord or its nerve roots so even a noncancerous growth can be disabling without treatment.
A spinal tumor is a benign or cancerous growth of cells in the spinal cord or surrounding areas. These tumors can compress the spinal cord or its nerve roots so even a noncancerous growth can be disabling without treatment.
What is a Tumor?
Cancers and tumors of the spine and spinal cord are relatively rare. The most common symptom that patients with a spinal tumor have is pain. Because back pain and neck pain are very common, it is also not a specific symptom of any one disease or medical condition. Luckily, most back and neck pain is not due to a tumor. However, if a cancer were discovered after a long period of “conservative” management of back pain, most patients would feel that their problem should have been investigated more thoroughly in the beginning. Therefore, the challenge is to determine how to evaluate back pain with the goal of specifically excluding a tumor as the cause of the pain.
What Are The Symptoms of a Tumor?
Pain symptoms that may suggest that a tumor or a cancer is responsible for the pain include pain that continues to get worse despite treatment, and that may be associated with other symptoms such as fatigue or weight loss. The pain may be worse at night, and not necessarily be related to level of activity. When associated with neurological symptoms such as loss of bowel and bladder control or pain running down the legs, further evaluation is clearly warranted. Be aware of other physical symptoms, such as lumps and bumps, moles on the skin, and any other findings that might suggest that you have a tumor somewhere else in your body.
Risk Factors
Most of us are aware of some of the risk factors that are associated with cancer in the United States. Cigarette smoking, an unhealthy diet, chemical and radiation exposure, a family history of certain cancers such as breast cancer or ovarian cancer, and over-exposure to the sun are common risk factors for certain cancers. These cancers generally occur in different parts of the body and then spread to the spine only after the cancer has been growing for a long period of time. The spine and vertebral bodies have a rich blood supply and cancer cells can spread to this part of the body by traveling in the bloodstream. Back pain is usually not the first symptom of a malignant cancer growing somewhere else in your body. Because of this fact, providers use routine medical tests in order to find certain cancers before they have a chance to spread instead of evaluating every patient with back pain as if they might have a cancer. Regular mammograms to look for breast cancers, pap smears to look for cervical cancer, chest x-rays to look for lung cancers, and fecal occult blood tests for colon cancers should be part of everyone’s health maintenance program.
How Is A Tumor Diagnosed?
Most spine tumors are found as part of a routine diagnostic evaluation for neck or back pain. This begins with a complete physical exam. If you have concerns that you may have cancer elsewhere, you should discuss this with your spine surgeon who will be able to help you make sure that you are getting the right tests. X-rays of your neck or back are always the initial step in the imaging process. X-rays are a very good way to look at the spine, but they are not foolproof. While many tumors will be visible on regular x-rays, some are much more difficult to see. This is especially true for those cancers involving the soft tissues such as the spinal cord itself or the muscles that surround the spine. When there are reasons to suggest that a cancer may be the cause of back pain, providers will usually order a bone scan, a CT scan (CAT scan), or an MRI. The combination of a history and physical exam, and the appropriate imaging studies will usually find or exclude the majority of spinal tumors.
How is a Tumor Treated?
The type of tumor, the extent of involvement of the vertebrae, the location, and the prognosis for the patient are all used to decide what type of treatment is best. Many times, this decision is made by a team of surgeons, oncologists, radiologists and other providers who specialize in taking care of patients with cancer. Many spinal tumors can be treated with very good results, and the pain can also be significantly alleviated. It is very important that you gather as much information as possible about the treatment options for the specific type of cancer that you or your loved one has. The first step in gathering this information is to make sure that you understand what type of cancer you are dealing with, and what your treatment options are. With this knowledge, you can actively participate in the decision making process with your team of providers.
Benign Tumors:
Providerss use the term “benign” to indicate that a particular tumor is unlikely to spread to others parts of the body. Benign tumors can still be a significant problem however, depending upon their location, size, adjacent structures, blood supply, and other factors. Fortunately, most benign tumors can be treated successfully.
The following are examples of benign tumors that can affect the spine and its surrounding structures:
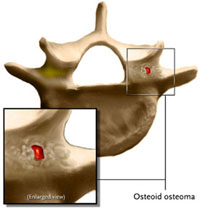
Osteoid Osteomas:
An osteoid osteoma is a benign lesion that has a unique tendency to affect the posterior part of the vertebra during adolescence. It occurs primarily in the pedicle and the posterior elements, not in the vertebral body. It accounts for about 10% of all bone tumors involving the spine. It typically presents as unrelenting pain, clearly worse at night, which is exquisitely sensitive to aspirin or Non-Steroidal Anti-inflammatory Drugs (NSAID’s) like Ibuprophen. It may be difficult to see on plain x-rays, but a bone scan is highly diagnostic. Treatment options include prolonged management with NSAID’s until the lesion eventually “burns out”, surgical excision, and a new treatment method using radio-frequency ablation. With surgery or ablation, pain relief is rapid and recurrence is rare.
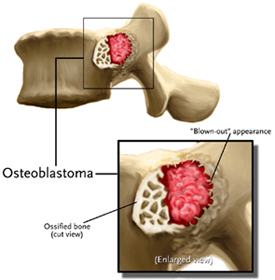 Osteblastomas:
Osteblastomas:
Osteblastomas are bigger versions of osteoid osteomas, and by definition, are greater than 2 cm in diameter. They also have the tendency to affect the posterior part of the spine and present with pain. They tend to be more aggressive and usually require surgical resection. Recurrence rates are higher than those seen with osteoid osteomas, meaning that they can come back in the same place about 10% of the time.
Aneurysmal Bone Cysts:
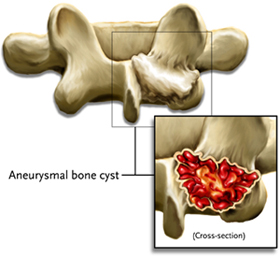
ABC’s are benign tumors that occur frequently in the cervical spine and may affect the posterior elements of the spine or the vertebral body itself. These tumors tend to affect older adolescents, presenting with pain and in some cases, neurological symptoms. The cause is poorly understood. The recommended treatment is excision and curettage of the lesion and decompression of the spinal elements when needed.
Giant Cell Tumors:
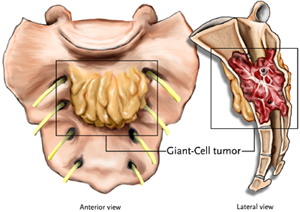
Giant Cell Tumors are poorly understood. They tend to affect the vertebral body (front of the spine), and despite being technically “benign”, they can be very aggressive and sometimes spread elsewhere. They may present with local pain as well as spinal cord compression symptoms. The most common age is between 20-40 years old, but this is variable. Treatment is generally surgical, with en-bloc (complete) resection being the preferred choice. There are some instances where radiation and pre-operative embolization of the tumor will improve the surgical risk and outcome. These tumors require careful pre-operative planning and a team approach before the initial surgical procedure. Incomplete removal of a vertebral giant cell tumor can lead to possible malignant transformation.
Eosinophilic Granuloma:
EG is a benign lesion of bone that will present with pain and the characteristic radiographic finding of “vertebra plana,” a collapse or flattening of the vertebral body and occurs in both children and adults. These tumors may occur by themselves, or as part of a syndrome involving multiple bones and other organs. Treatment decisions are highly individualized with no clear consensus on the “best” method of treatment. Many of these tumors can be managed without surgery, or in certain cases, low dose radiation.
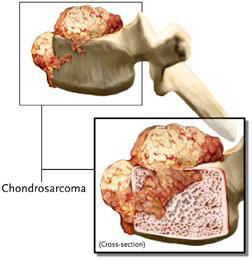
Enchondromas:
Enchondromas are benign tumors made of cartilage. They have the potential to enlarge to the point of impinging on the spinal canal or neural elements. When symptomatic, the recommended treatment is surgical excision. There is a rare incidence of these tumors changing to a low-grade malignant cartilage tumor known as a chondrosarcoma. This is fortunately quite rare, but a rapid increase in size may warrant biopsy of the lesion. Providerss use the term “malignant” to indicate that a particular tumor or a cancer often spreads to other parts of the body, and can be difficult to cure or treat. This is very different from “benign” cancers, which are much less likely to spread, are easier to treat and control.
Malignant Tumors:
Providerss use the term “malignant” to indicate that a particular tumor or a cancer often spreads to other parts of the body, and can be difficult to cure or treat. This is very different from “benign” cancers, which are much less likely to spread, are easier to treat and control.
The following are examples of malignant tumors that can affect the spine and its surrounding structures.
Metastatic disease:
Any malignant tumor can metastasize to bone, but the most common sites are the breast, prostate gland, kidney, thyroid, and lung. The two ways tumor cells can reach the vertebral column are by the venous system and the arterial system. The spine and its surrounding elements have a generous blood supply, draining many of the structures of the lower abdominal cavity via a system of veins called Batson’s Plexus. The lymphatic channels are also considered a third but less probable way.
The spread or metastasis of tumors from elsewhere in the body to the spine may occur after a cancer has been growing in another part of the body for a long time. Tumors that have spread to the spine usually cause a significant amount of pain. If they are large enough, they may put pressure on the spinal cord, which causes increasing pain and loss of normal functioning in the bowel, bladder, and legs. Metastatic cancer may not be curable, but the treatment goals are usually directed at relief from pain, decompression of the neural elements (removing the pressure on the spinal cord and nerves), and preserving the patient’s quality of life as much as possible. Surgery, chemotherapy, and localized radiation therapy all play a role in reducing the pain associated with cancers that have spread to the spine from other sites.
 Myeloma:
Myeloma:
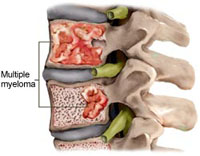
Myeloma is the most common primary malignant tumor of bone. It typically affects adults greater than 40 years of age. It tends to be generalized, involving multiple bones, but pain and involvement of the spine is the most common presenting complaint. The majority of patients have vertebral involvement while a fewer number have vertebral pain. Treatment is palliative meaning that disease can be controlled, but not completely cured. Chemotherapy is used to control the pain and slow the progression of the disease. Surgery may be required if pathological fractures develop or there is compression of the spinal cord.
 Osteosarcoma:
Osteosarcoma:
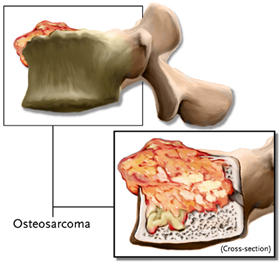
Osteosarcoma is the second most common primary malignant tumor of bone. There are two age groups that most often develop this type of cancer. It typically affects adolescents and young adults, with a second peak of incidence in older adults. It is very rare in the spine. Modern advances in imaging, chemotherapy, and surgical treatment of osteosarcoma have significantly improved the 5-year survival to greater than 80 percent. This is an amazing accomplishment, since 20 years ago this disease was almost always fatal.
Leukemia:
Leukemia, in its many forms, may present with back or neck pain, which can be caused by the cancer growing in the bone marrow of the vertebral body. However, the more common symptoms of leukemia, such as fevers, fatigue, bruising, excessive bleeding, and anemia are usually noticed well before spine pain occurs.